Reverse shoulder replacement has changed the game for patients with rotator cuff arthropathy, massive cuff tears, severe arthritis with bone loss, and certain complex shoulder fractures. This procedure has offered meaningful pain relief and a return to daily activities for many patients over the years. However, like any surgery, it comes with potential risks. Understanding the potential problems with reverse shoulder replacement is an important first step in preventing them. In this post, we’ll walk you through the most common problems with reverse shoulder replacement, explain what causes them, and explore how thoughtful surgical planning and advanced implant design may help reduce your risk.
Key Takeaways
- The most commonly reported problems include instability or dislocation, scapular notching, infection, nerve injury, acromial fractures, and component loosening.
- Implant design plays a role in complication prevention. Lateralized designs are engineered to help reduce issues such as scapular notching and instability.
- Pre-surgical planning tools may help surgeons optimize implant positioning for each patient’s unique anatomy.
- Patient actions before and after surgery, such as managing health conditions, following rehabilitation protocols, and communicating openly with your surgeon, can also help minimize risk.
What Is a Reverse Shoulder Replacement?
Your shoulder is a ball-and-socket joint. In a healthy shoulder, the ball sits on top of the upper arm bone (humerus) and fits into the socket on the shoulder blade (glenoid). A group of tendons known as the rotator cuff stabilizes the joint and helps generate movement.
When the rotator cuff is severely damaged or torn beyond repair, a traditional shoulder replacement often cannot function properly. The joint may remain unstable. That is where a reverse shoulder replacement comes in.
In a reverse shoulder replacement, the surgeon essentially flips the anatomy. The ball component gets placed on the glenoid (shoulder blade side), and the socket component goes on the humeral (arm bone) side. This “reversed” configuration allows the deltoid muscle, rather than the damaged rotator cuff, to power shoulder movement.
Reverse shoulder replacement may be recommended for cuff tear arthropathy, irreparable rotator cuff tears, certain complex shoulder fractures, and as a revision to prior shoulder replacements.
Common Problems with Reverse Shoulder Replacement
While reverse shoulder replacement is generally a low-risk procedure, no surgery is without risk, and reverse shoulder replacement is no exception. Understanding the potential issues can help you feel more prepared and empowered going into your procedure. In the following subsections, we’ll review the most frequently discussed problems with reverse shoulder replacement.
Implant Instability and Dislocation
Dislocation, where the implant components separate, is among the reported complications after reverse shoulder replacement. Contributing factors may include inadequate soft tissue tension, improper component positioning, or patient-related risk factors. Many dislocations can be treated with closed reduction and temporary immobilization, though recurrent instability or implant-related factors may require additional intervention.
Scapular Notching
Scapular notching is a complication that occurs when the humeral component repeatedly contacts the scapular neck during movement, gradually wearing away bone over time. Older implant designs with a more medialized center of rotation tended to show higher rates of notching. While mild notching may not cause noticeable symptoms, more severe cases have been associated with decreased function and potential implant loosening. Newer, lateralized designs have been developed in part to help address this problem.
Infection
Infection is a risk with any surgical procedure. Certain bacteria, including organisms that naturally live on the skin around the shoulder, are particularly relevant in shoulder surgery. Treatment typically involves antibiotics, and in some cases, additional surgery to wash out the joint or revise the implant.
Nerve Injury
The axillary nerve and brachial plexus are the structures most commonly affected during reverse shoulder replacement. Nerve injury can result from retraction, manipulation, or the relative lengthening of the arm that occurs with the procedure. Many nerve injuries are temporary and tend to resolve over weeks to months.
Acromial and Scapular Spine Fractures
Stress fractures of the acromion or scapular spine may develop after surgery due to increased stress on these bony structures from the changed biomechanics of the reversed construct. Patients with osteoporosis or pre-existing acromioclavicular joint arthritis may face a higher risk.
Component Loosening
Over time, the implant components can potentially loosen from the bone. Loosening on the glenoid side (the baseplate) has historically been a concern, particularly with certain fixation designs. Strong initial fixation and proper implant positioning are considered important in helping prevent this complication.
How Implant Design Helps Prevent Complications
One of the most exciting developments in reverse shoulder replacement over the past decade has been the evolution of implant design. The original reverse shoulder prosthesis was a groundbreaking achievement. It medialized the center of rotation and relied on the deltoid for arm elevation, which worked well for many patients.
However, the design was associated with certain drawbacks that prompted engineers and surgeons to look for design-based solutions. This is where the concept of lateralization enters the picture.
Understanding Lateralization
Lateralization refers to shifting the center of rotation of the shoulder joint outward (laterally) from where the original design placed it. Research has shown that lateralized designs may offer several potential advantages. Lateralized designs have been associated with lower reported rates of scapular notching and may help restore a more natural shoulder contour. Some studies suggest improvements in rotational range of motion, particularly external rotation.
That said, lateralization is not a one-size-fits-all solution. Too much lateralization can increase stress on the glenoid fixation or cause impingement in other areas. Finding the right balance for each patient is where surgical expertise and proper planning become essential.
The InSet® Reverse Shoulder System: A Closer Look
In my practice, I often use the InSet® Reverse Shoulder System by Shoulder Innovations. This system was designed with a specific question in mind: how could a reverse shoulder replacement behave more like an anatomic shoulder? That philosophy drives many of the system’s design features and helps inform my approach to preventing problems with reverse shoulder replacement for my patients.
Lateralized Glenoid and Humeral Design
The InSet® system offers a lateralized glenoid and lateralized humerus construct. This bipolar approach to lateralization is designed to improve rotational capacity by positioning the greater tuberosity in a way that may support post-operative function.
On the humeral side, the InSet® system provides multiple stem options. When paired with the lateralized glenoid offering, this combination is intended to support refined biomechanics and enhanced range of motion while potentially minimizing certain post-operative complications.
Versatile Baseplate Options
The InSet® system features baseplates in a range of configurations. This range allows surgeons to address varying degrees of glenoid bone loss or deformity. A well-fixed and properly positioned baseplate is one of the foundations of a long-lasting reverse shoulder replacement.
Titanium Porous Coating for Fixation
Implant longevity often depends on how well the component bonds with the surrounding bone over time. The InSet® titanium humeral stems feature proprietary curved fins coated with a porous titanium material designed to promote bone ingrowth and biological fixation. This combination aims to enhance both rotational stability and long-term fixation while preserving as much bone as possible, an important consideration should a revision ever become necessary down the road.
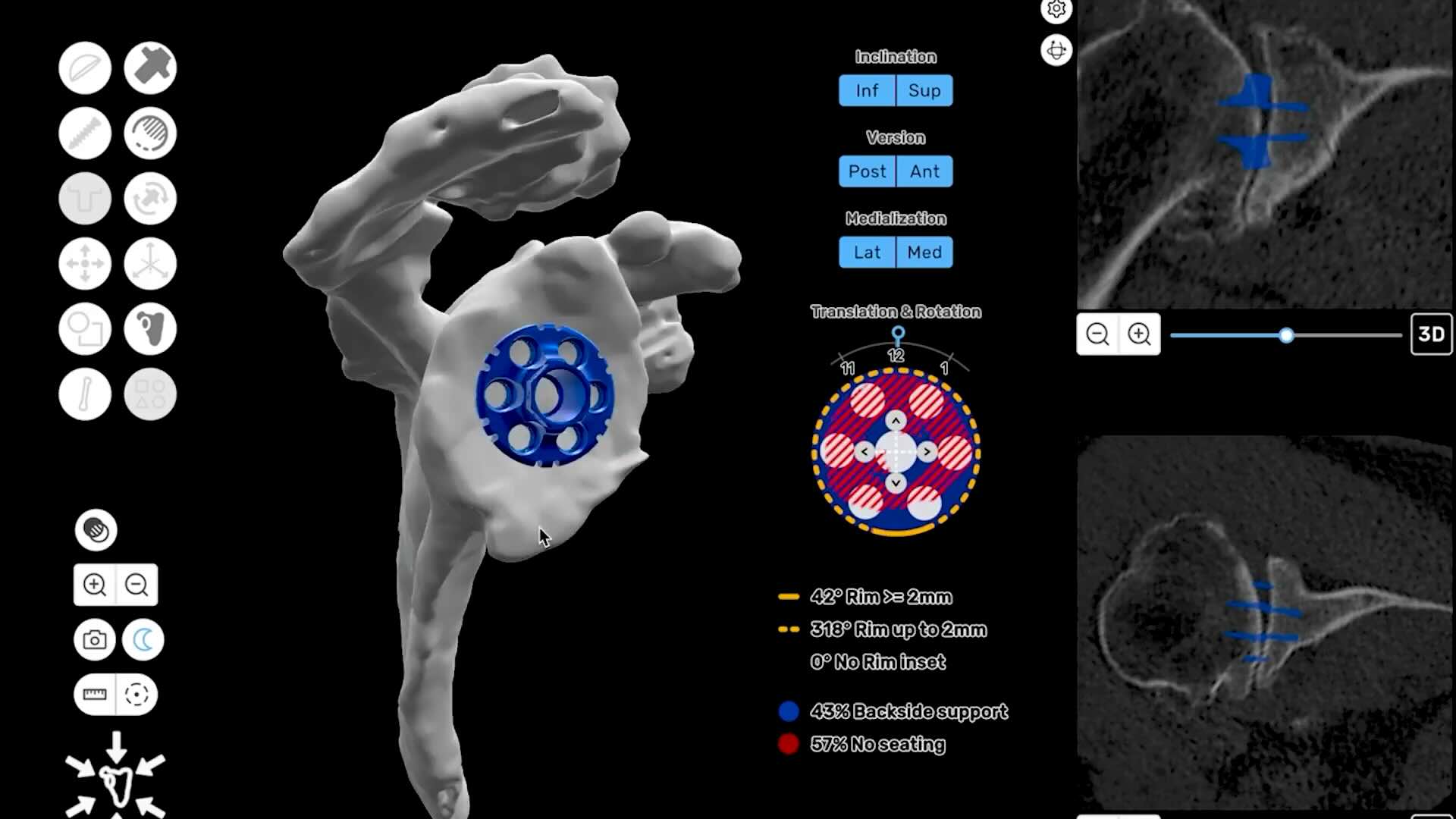
Pre-Surgical Planning
Proper implant placement is one of the key factors in helping prevent complications. ProVoyance® is a shoulder planning software that converts a patient’s CT scan into a three-dimensional computerized model. This allows the surgeon to evaluate bone quality, plan component positioning, and anticipate potential challenges before stepping into the operating room.
What You Can Do to Reduce Your Risk
While implant design and surgical technique are important, patients also play an active role in preventing problems with reverse shoulder replacement. Here are some steps that may help set you up for a better outcome:
- Manage your overall health before surgery. Certain conditions, along with lifestyle factors like smoking, can increase complication risk. Working with your doctor to optimize these factors ahead of time is recommended.
- Be honest about your medical history. Let your surgeon know about prior surgeries, infections, medications, and any health conditions. This information helps with surgical planning.
- Follow your rehabilitation plan. Physical therapy is usually a component of recovery after reverse shoulder replacement. Sticking to the prescribed protocol, and not pushing too hard too fast, can help protect your new joint.
- Attend all follow-up appointments. Regular check-ins with your surgeon allow for early detection of any issues, such as component loosening or subtle fractures that may not be immediately apparent.
- Communicate openly. If something does not feel right during recovery, speak up. Early intervention is generally more effective than waiting for a problem to progress.
Choosing an experienced shoulder surgeon who specializes in shoulder replacement and uses modern implant technology is another meaningful step. Fellowship training, surgical experience, and familiarity with implant systems and planning tools are important factors in preoperative preparation and intraoperative decision-making.
Summary
Reverse shoulder replacement is a procedure that has improved the quality of life for countless patients dealing with rotator cuff arthropathy, massive cuff tears, complex fractures, and failed prior replacements. While problems with reverse shoulder replacement do occur, ongoing refinements in implant design and surgical technique continue to be studied with the goal of improving outcomes and reducing complications over time.
Lateralized implant designs represent a step forward in addressing some of the historical challenges of reverse shoulder replacement, including scapular notching, limited rotation, and instability. Combined with thorough pre-surgical planning using tools, these innovations may help surgeons deliver more precise, personalized care.
Frequently Asked Questions
What is the recovery timeline for reverse shoulder replacement?
Timelines vary, but many patients can expect to wear a sling for approximately two to three weeks after surgery. Physical therapy typically begins within the first few weeks and continues for several months. Many patients see meaningful improvements in pain and function within three to six months, though full recovery may take up to a year or longer.
Can reverse shoulder replacement be done as an outpatient procedure?
In most cases, yes. Depending on the patient’s overall health, the complexity of the procedure, and the surgical facility, reverse shoulder replacement may be performed as an outpatient surgery with the patient going home the same day. Your surgeon will help determine the best plan for your specific situation.
How do I know if I am a candidate for reverse shoulder replacement?
Reverse shoulder replacement is typically recommended for patients with rotator cuff arthropathy, irreparable cuff tears, severe arthritis with bone loss, certain complex fractures, and failed prior shoulder replacements. A thorough evaluation by a shoulder specialist is the best way to determine if this procedure is right for you.
